5 Comments
On the whole, we will continue to provide timely and targeted support for all of our patients and their families in any way possible to help decrease anxiety or other mental health concerns related to this public health event. We will be here to support you as these events unfold. Please be aware that only an extremely small segment of the US population will have a serious impact from the virus. Many of our patients are considered to be at very low risk for a serious impact.
Feel free to contact me directly if you have any questions about how your specific treater or any of our staff can help you through these challenging times. Our procedures are based upon Massachusetts public health procedures and federal guidelines that are distributed via the Centers for Disease Control. The overriding goal of this letter is to promote hygiene and not to increase anxiety. You can refer to the links listed at the end of this post for additional information.
Practical health behaviors that we have implemented to minimize transmission:
Informing us of Risk Factors:
At the onset of each session:
Grief Support:
What if your clinician becomes ill?
I thank you for taking the time to review our concerns and response to this global health event. As is always the case, the support that we provide to each other and the manner by which we work together during these trying moments will help us define who we are in these times of uncertainty. My staff and I all look forward to passing the most critical test during these times, the test of our compassion for others during times of need. Be well and remain as healthy as possible. Sincerely, Dr. Perna David A. Perna, PhD President, Copernican Clinical Services Lecturer in Psychology, Department of Psychiatry Harvard Medical School Helpful Links: How to prepare for Coronavirus in your:
American Psychological Association Podcast on Coronavirus and anxiety: Bloomberg-How Quarantines Have Impacted Mental Health in China: Psychiatric Times Article-Coronavirus and its Impact on Global Mental Health: Thanh Phan, MA, our Psychology Intern from William James College, helps launch the Asian Mental Health Concentration
Thanh Phan, MA, our Psychology Intern, had asked me if Copernican Clinical Services (CCS) would help sponsor the launch of William James College's Asian Mental Health Concentration (AMHC). I told her that we would all be thrilled to do so.

Faculty, students, and family members were enthusiastically engaged in the launch and the Lunar New Year celebration
Acculturation:
|
||||||||||||||||||||||||||||||||||||||||||||||||










Mentoring: Thanh has been mentored by Dr. Catherine Vuky, PhD, the Director of the Asian Mental Health Concentration at William James who is also a staff psychologist at The South Cove Community Health Center in Boston. Dr. Vuky and Thanh make a great duo. It is easy to see why Thanh has such a sense of hope for the future of the AMHC. That future burns so brightly in the eyes of Dr. Vuky every day and is only matched by her warm smile and sense of commitment to her work. I am glad to see that they both have so much energy. The road ahead is long-so the company you keep makes all the difference. |

Catherine Vuky, PhD
|
Please click on the following Links for more information:
 David A. Perna, PhD |  |
Categories All "Anger Follows a Developmental Trajectory"  "We use the CBT framework for our anger |  Staff at the Yale Child Study Center have provided a helpful summary Article on how to differentiate between anger, irritability, and aggression. I think that it is one of the better summary articles that I have come across in the last year. While it covers a variety of topics that have been discussed in the past, it does so with a sense of clarity that fellow authors seem to lack. Here are a list of the points that I think were helpful:
Sukhodolsky offers his version of treatment which has proven to be clinically effective in a research environment. It is a sophisticated treatment model that is thoughtful and has withstood randomized treatment trials. However, like many of these manual-based, highly structured research protocols one can easily ask, "What is the clinical relevance of this research, when one applies it to a typical outpatient treatment environment?" I do think that reading this type of research can be helpful in guiding clinicians to adopt "best practices" that help with anger management treatment. However, out-patient treatment of anger is complicated and at times sequentially confusing for both the patient and the inexperienced clinician. I do find it surprising that Sukhodolsky comments that CBT is generally implemented on a one-on-one basis. He seems to miss the fact that many models of anger management are based on group models that rely on CBT frameworks. We use the CBT framework for our anger management groups. Overall I give the article two thumbs up. Kudos to the staff at Yale! Dr. Perna |

Categories All "Dyslexia affects many brain regions, not just those involved with language." 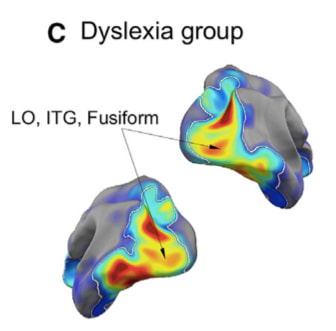 | MIT Researcher John Gabrieli published fascinating findings in the journal Neuron as part of his research and the research of his team (See Reference below) into the roots of dyslexia. His research revealed that dyslexia impacts many different systems within the brain which in turn impact the ability of the dyslexic child to adapt to his/her environment. Gabrieli also noted:
I found this article fits my clinical impressions of the complex nature of many child and adolescent patients who struggle with dyslexia. It also highlights the numerous systems that we need to address in our treatment in an applied clinical setting with this population. In our work, we commonly address the degree to which these patients struggle with anger outbursts, poor frustration tolerance, and impulsivity, all of which bring them to our door for treatment. In treating such a complex population, our treatment interventions are equally complex, including familial support, school support, self-esteem support, referral for specialized testing (Such as Central Auditory Processing Evaluations), and individual/family therapy that are all intertwined to address each patients specific learning/mental health concerns. It is beyond the scope of this review to reveal the complexity of this MIT team's work in this area. A thorough reading of the article that is listed below is recommended. Perrachione et al., 2016, Neuron 92, 1383–1397 December 21, 2016 |
  |  Image From the New York Times |
Categories All | Here is the 2014 New York Times article that many educators have asked me to forward to them. It focuses on the differences in note taking with a pen vs. keyboarding on a computer. It talks about:
Please feel free to look at Dr. Mueller and Oppenheimer's academic article: Mueller, P., & Oppenheimer D. M. (2014). The Pen Is Mightier Than the Keyboard: Advantages of Longhand Over Laptop Note Taking. Psychological Science, Vol. 25(6) 1159–1168
Here is the link to the original New York Times article that was written by reporter Laura Papano: Take Notes From the Pros (2014, October 31) The New York Times, Retrieved From http://nytimes.com | ||
 David A. Perna, PhD |  |
"Executive functions are viewed to be primary learning challenges that impact functioning across a variety of learning contexts." | Many children with anger issues suffer from executive function deficits. These deficits impact their ability to make effective academic progress in school in addition to impacting their functioning in a variety of other social-learning contexts. Executive functions are viewed to be primary learning challenges that impact functioning across a variety of learning contexts. Unlike a specific learning disability, such as dyslexia, which is viewed to impact a specific learning category, such as reading, an executive function deficit generally, impacts multiple categories of learning. For example, an attention deficit disorder would impact an individual’s ability to make progress in many learning categories, whether they are academic or social. The inability to pay attention in class can impact the ability to learn history as well as the ability to drive a car safely. Organizational deficits are pervasive as well. For example, the inability to organize one’s assignment pad would impact school performance, while it could also impact the ability to socialize with friends (calling friends to get together too late on a friday night rather than earlier in the week). |
"Cognitive flexibility allows kids to adjust to the curve balls that life throws at them." | Common Executive Function Deficits Associated with Anger Management Disorders: 1. Causal Linking Challenges: The inability to understand that one event causes the other. An example would be a patient who thinks that his probation officer is causing him to have a limited social life, forgetting the fact that the probation officer was assigned to work with him because he had made the poor choice of assaulting another person. In this situation the patient loses track of his own behavior as the primary reason why he has lost many age-appropriate freedoms. Within school it might include the lack of understanding that completing homework will increase one’s understanding of the class material and subsequent performance on tests. 2. Organizational Deficits: Difficulties with the ability to keep track of details that allow the patient to successfully negotiate a myriad of social interactions and learning opportunities. An adolescent might be upset that she has misplaced her homework assignment and cannot complete her homework. However, within her social interactions she might become angry at a parents when she misplaces a slip of paper that contained a phone number that she felt was essential to her social life. 3. Sequencing Challenges: Difficulties with the ability to keep track of sequences of events that are needed to facilitate a positive outcome in a learning situation. The inability to follow a given sequence to solve a math problem will generally result in the wrong answer. In a job situation, an adolescent might sanitize the counters of a fast-food establishment and then place a package with raw chicken onto the cleaned counter in front of his boss just prior to being terminated. A hard-working kid would have lost a job over the likelihood that his sequencing challenge could result in someone going to the hospital. 4. Time Management Issues: Difficulties with allocating time to complete/attend events and activities that are of meaning to the patient or other people in his/her environment. An example would include having an adolescent plan on completing a major project for school on a weekend when relatives were visiting from out of town resulting in a huge family fight. Within the social realm it might include being bombarded by complaints from peers as a result of being late for a movie. 5. Transition Issues: Difficulties with the ability to transition between two activities. Examples of these difficulties range from obvious difficult transitions, such as ending summer and starting school in September to less clear transitions, such as the movement from a sleeping state to a waking state each morning. The resulting morning tirades can be overwhelming for parents. Within a middle school environment the process by which kids constantly move from class to class could prompt a student with this challenge to feel unsettled throughout the school day. As soon as he feels settled in class the bell rings and he has to head off to the next one. As the day progresses the sense of stress increases to the point where an explosion can occur in the last period of the day. 6. Cognitive Flexibility: The ability to learn new ways of coping with ever-changing stressors in a fluid manner. This issue is many times referred to as the ability to be prepared for all of the “Curve balls” that life throws one’s way. A child who was taught one way of solving a math problem using long division in 5th grade becomes enraged when her 6th grade teacher introduces a new method. Or in social settings it might represent the ability to quickly respond to the fickle interests of a peer group who wanted to go to the mall on Friday night when plans were made earlier that day during school lunch, to the movies when plans were made at 6PM Friday night, and out for food at 9PM when all the peers at the theater realized that the popular kids were having dinner at a nearby Shake Shack. For the average teen popularity always tops planning, however, for the teen with cognitive flexibility issues the plan is written in stone. This skill challenge is closely tied to transitioning challenges and challenges in understanding other people’s perspectives (theory of mind). 7. Memory: The ability to remember information in a manner that allows it to be readily available for quick and efficient access. For example, a child might erupt at the thought that he had to get his hair cut when in fact both parents informed him of the hair cut days earlier. In school it might include the embarrassment of walking into class on a Monday morning and being handed a test by the teacher after forgetting to study over the weekend. 8. Generalization: The ability to generalize from one situation to the other. For example, a student is told not to write on his desk at school, which he agrees not to do, but is then caught writing on a table in the cafeteria. In such a situation the child may be incredibly frustrated that the teacher did not clarify this issue to a greater extent and may become highly focused on the fact that he has not written on his desk since the teacher asked him to stop. The connection between the two situations is simply not apparent to the student, while the teacher may start to feel that the student is playing him/her. In reality the student is simply clueless to the connection between the two contexts. |
Categories
All
1 David A. Perna
2 Caitlyn Chappell
3 Heather Corazzini
4 Alexis Chirban
Adolescent Psychology
Anger Management
Borderline Personality Disorder
Cultural Awareness
DBT Techniques
Diversity
Education
Executive Function
Healthy Lifestyles
Learning Challenges
Mindfulness
Nutrition
Social Media
Technology
Your Child
Youth Violence
 David A. Perna, PhD |  |
| For those who are interested in working with angry patients the journey is fascinating. However, from a countertransference perspective one needs to be cautious and should follow the advice that Nietzsche offers in Beyond Good and Evil: “He who fights with monsters should be careful lest he thereby become a monster” “And if thou gaze long into an abyss, the abyss will also gaze into thee” Let me be clear, the monster is not the patient, it is the anger and rage that he or she harbors. In his comments Nietzsche is referring to the extent that one can become tainted and reactive when interacting with such challenging behaviors over time. It is often all to easy to focus on the client’s overreactions and extreme rages and lose sight of the clinician's own clinical shortcomings and tendencies to be blind to his/her own hurtful behavior and countertransference blindspots. |
 Arc de Triomphe interior, statue- “La Marseillaise” Credit: David A. Perna (2014) | In working with angry patients one is constantly challenged to address one’s own temper and tendency to lash out in a sadistic/hurtful manner. Boundaries that seem to be so clear when one is in training under clinical supervision can at times become blurred later in a clinician's career during an intense treatment experience. The risk is the likelihood that the clinician can start to treat the patient with the same sense of venom and distrust that the patient experiences in his/her daily interactions. This is the slippery slope that prompts one to lose clinical perspective as the abyss grabs a hold and pulls the clinician downward.. One of Marsha Linehan's greatest contributions to the field of contemporary psychology has been her ability humanize the the treatment of patients diagnosed with Borderline Personality Disorder. This population has always been identified by treaters and members of the general population as angry and furious. Prior treatment approaches encouraged sadistic reactions to borderline patients who struggled with mood regulation skill challenges, rage, and a long history of interpersonal instability with significant others. Linehan's "Eastern Philosophical" approach to treatment posited that the therapist was at fault if the patient did not progress, thereby prompting the therapist to think of ways to change his/her approach rather than simply rebuking the patient as being lazy or slothful. This humanistic approach ushered in a much healthier era in treating Borderline patients by helping them develop skills in an incremental manner that is at times slow, and yet with time-steady and incrementally effective. So in following Nietzsche's lead, the clinician should always question him/herself when the interaction with the patient becomes intense. Anger and rage focused back towards the patient and family should always be considered as unhealthy and connected to the pull of the abyss. There have been so many clinicians who have rationalized these hurtful approaches as appropriate and needed in light of the patients acting out, but the truth is that they represent an unhealthy countertransference response to a vulnerable group of patients. |
 David A. Perna, PhD |  |
 "Parents Should Use Their Values to Guide Their Parenting" | Parents, educators and fellow clinicians have asked me the same question: "What impact does violent social media have upon my child/student/patient?" I recently had the opportunity to address this topic along with my colleague Liz Barcewicz, PsyD. We were asked by Court Booth, Director of Community Education in Concord-Carlise (He is also a LinkedIn Member), to speak about the impact of violent social media on our youth. We had the added pleasure of presenting at Concord-Carlisle's new high-tech high school. The school was only seven days old when we walked into the new multi-media center. Our primary talking points were as follows:
|
 "Help younger children by placing upsetting news stories into a larger context"
|
|
|
|
References: |
|