5 Comments
On the whole, we will continue to provide timely and targeted support for all of our patients and their families in any way possible to help decrease anxiety or other mental health concerns related to this public health event. We will be here to support you as these events unfold. Please be aware that only an extremely small segment of the US population will have a serious impact from the virus. Many of our patients are considered to be at very low risk for a serious impact.
Feel free to contact me directly if you have any questions about how your specific treater or any of our staff can help you through these challenging times. Our procedures are based upon Massachusetts public health procedures and federal guidelines that are distributed via the Centers for Disease Control. The overriding goal of this letter is to promote hygiene and not to increase anxiety. You can refer to the links listed at the end of this post for additional information.
Practical health behaviors that we have implemented to minimize transmission:
Informing us of Risk Factors:
At the onset of each session:
Grief Support:
What if your clinician becomes ill?
I thank you for taking the time to review our concerns and response to this global health event. As is always the case, the support that we provide to each other and the manner by which we work together during these trying moments will help us define who we are in these times of uncertainty. My staff and I all look forward to passing the most critical test during these times, the test of our compassion for others during times of need. Be well and remain as healthy as possible. Sincerely, Dr. Perna David A. Perna, PhD President, Copernican Clinical Services Lecturer in Psychology, Department of Psychiatry Harvard Medical School Helpful Links: How to prepare for Coronavirus in your:
American Psychological Association Podcast on Coronavirus and anxiety: Bloomberg-How Quarantines Have Impacted Mental Health in China: Psychiatric Times Article-Coronavirus and its Impact on Global Mental Health: Home Schooling Strategies-Mindful Parenting: Part 1 Embracing the Moment: Being with your child3/8/2020
 Keep an eye out for future posts on specific applications of mindfulness activities for during the current health crisis. Be healthy and be strong. References: Coatsworth, J. D., Duncan, L. G., Nix, R. L., Greenberg, M. T., Gayles, J. G., Bamberger, K. T., … Demi, M. A. (2015). Integrating mindfulness with parent training: Effects of the mindfulness-enhanced strengthening families program. Developmental Psychology, 51(1), 26–35. doi: 10.1037/a0038212 Deng, Y., Zhang, B., Zheng, X., Liu, Y., Wang, X., & Zhou, C. (2019). The role of mindfulness and self-control in the relationship between mind-wandering and metacognition. Personality and Individual Differences, 141, 51–56. doi: 10.1016/j.paid.2018.12.020 Geronimi, E. M. C., Arellano, B., & Woodruff-Borden, J. (2019). Relating mindfulness and executive function in children. Clinical Child Psychology and Psychiatry, 135910451983373. doi: 10.1177/1359104519833737  Categories All Thanh Phan, MA, our Psychology Intern from William James College, helps launch the Asian Mental Health Concentration
Thanh Phan, MA, our Psychology Intern, had asked me if Copernican Clinical Services (CCS) would help sponsor the launch of William James College's Asian Mental Health Concentration (AMHC). I told her that we would all be thrilled to do so.

Faculty, students, and family members were enthusiastically engaged in the launch and the Lunar New Year celebration
Acculturation:
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||















Mentoring: Thanh has been mentored by Dr. Catherine Vuky, PhD, the Director of the Asian Mental Health Concentration at William James who is also a staff psychologist at The South Cove Community Health Center in Boston. Dr. Vuky and Thanh make a great duo. It is easy to see why Thanh has such a sense of hope for the future of the AMHC. That future burns so brightly in the eyes of Dr. Vuky every day and is only matched by her warm smile and sense of commitment to her work. I am glad to see that they both have so much energy. The road ahead is long-so the company you keep makes all the difference. |

Catherine Vuky, PhD
|
Please click on the following Links for more information:


Categories All  "There isn’t one single reason eating disorders begin or are maintained"  "For some kids certain food textures make them feel like someone is dragging their nails across a blackboard"  “perfectionistic language” is a common trait shared  | Does your adolescent’s eating behavior, weight, or exercise ever appear abnormal to you? Do they seem preoccupied with their physical appearance? Have you considered asking them about it, but weren’t sure how to approach them? Not all eating patterns or behaviors would constitute an eating disorder diagnosis; however, disordered eating patterns and behaviors are real, require careful consideration, and can have serious health implications. Trust Your Intuition: Eating disorders are often disguised in ways that minimize their significance. At times they can be difficult to assess and are often overlooked by adults. If your intuition as a parent tells you something might be “off,” with your child’s eating, listen to it, and consult a professional for guidance. It’s okay to be unsure about what you have noticed. Speaking with a mental health professional who has experience in this area can help you develop language that will allow you to express your intuitions to your child in a clear and supportive way. Eating Disorders can be Deadly: The prevalence of adolescent eating disorders has gained significant attention in the mental health field over the last decade. Some researchers have claimed anorexia nervosa has the highest mortality rate of all psychological disorders (NEDA, 2018). See: https://www.nationaleatingdisorders.org for more information. How does it Start? Many parents ask, “How did this start? Why and when did my child become so obsessed with what they’re eating?” Studies offer arguments for why and how eating disorders are developed and maintained. In 2016, a team of researchers examined risk factors they believed to predict onset of eating disorders in adolescent females. According to their study, adolescent females were most at risk to develop eating disorders if they dieted, idealized thinness, had body dissatisfaction, and displayed unhealthy weight control behaviors (Stice et al., 2016). Despite research supporting specific reasons for ED development and maintenance, it can be argued such reasons are multifactorial;there isn’t one single reason eating disorders begin or are maintained. Eating disorders may also function as a form of self-punishment, manifestation of anxiety, or addiction—with little to no emphasis on weight loss as a central goal. Sensory Integration Issues: Not all eating disorders develop from preoccupation with fear of weight gain. Aversion to texture, fear of choking, fear of swallowing, etc., can also develop into ED (see Avoidant Restrictive Food Intake Disorder, DSM-5 criteria that are listed below). · An eating or feeding disturbance (e.g., apparent lack of interest in eating or food; avoidance based on the sensory characteristics of food; concern about aversive consequences of eating) as manifested by persistent failure to meet appropriate nutritional and/or energy needs associated with one (or more) of the following:
https://www.nationaleatingdisorders.org/learn/by-eating-disorder/arfid Many children who struggle with sensory integration disorders have difficulties with their eating, due to their reactivity to strong odors/tastes and certain textures of food. Their eating issues can often be compounded by the presence of muscular weaknesses in their mouth, tongue, and throat that impair their ability to swallow food. One researcher stated… “Often when kids display picky eating, especially those with food aversions/extreme picky eating, the touch, taste, or smell of a food is being processed in their brain as dis-pleasurable in some way. And, by dis-pleasurable, I mean down-right uncomfortable. Think of something that makes you shutter… nails on chalkboard or touching a slug?” (Grogan, 2018) See: https://yourkidstable.com/sensory-processing-and-picky-eating/ What about Boys? According to the National Eating Disorders Association (NEDA), approximately 0.3 – 0.4% of young women and 0.1% of young men will suffer from anorexia nervosa. Despite the common assumption eating disorders are exclusive to women, NEDA claims 25% of individuals with anorexia nervosa are male. Additionally, NEDA claims disordered eating behaviors (binge-eating, purging, laxative abuse, fasting) are nearly equal across male/female genders. For example, many boys who wrestle in high school manage their calories and exercise level so they can “cut weight” before a wrestling match. Additionally, dehydration can cause poorer performance in these athletes and places them at risk for more serious health concerns. See: http://pediatrics.aappublications.org/content/140/3/e20171871 Regardless of the severity of source of the ED, the way you communicate about this with your child matters! Researchers in 2011 conducted a study addressing the relationship between adolescent disordered eating and parent-child communication dynamics. The researchers concluded individuals’ thoughts of defectiveness, failure, and unrelenting standards from their parents contributed to their eating disorder. Findings suggest “perfectionistic language” is a common trait shared between parents and adolescents with disordered eating (Deas et al., 2011). “Perfectionistic language,” looks different within each family. Do NOT:
Parents are encouraged to alter their communication style in ways that may discourage the onset or maintenance of an eating disorder. Do try to:
Try not to forget: It is your child, so it’s up to you.-Notice, listen, and speak up. References: Deas, S., Power, K., Collin, P., Yellowlees, A., & Grierson, D. (2011). The relationship between disordered eating, perceived parenting, and perfectionistic schemas. Cognitive Therapy And Research, 35(5), 414-424. Stice, E., Gau, J. M., Rohde, P., & Shaw, H. (2017). Risk factors that predict future onset of each DSM-5 eating disorder: Predictive specificity in high-risk adolescent females. Journal Of Abnormal Psychology, 126(1), 38–51. |
 David A. Perna, PhD |  |
Categories All "Anger Follows a Developmental Trajectory"  "We use the CBT framework for our anger |  Staff at the Yale Child Study Center have provided a helpful summary Article on how to differentiate between anger, irritability, and aggression. I think that it is one of the better summary articles that I have come across in the last year. While it covers a variety of topics that have been discussed in the past, it does so with a sense of clarity that fellow authors seem to lack. Here are a list of the points that I think were helpful:
Sukhodolsky offers his version of treatment which has proven to be clinically effective in a research environment. It is a sophisticated treatment model that is thoughtful and has withstood randomized treatment trials. However, like many of these manual-based, highly structured research protocols one can easily ask, "What is the clinical relevance of this research, when one applies it to a typical outpatient treatment environment?" I do think that reading this type of research can be helpful in guiding clinicians to adopt "best practices" that help with anger management treatment. However, out-patient treatment of anger is complicated and at times sequentially confusing for both the patient and the inexperienced clinician. I do find it surprising that Sukhodolsky comments that CBT is generally implemented on a one-on-one basis. He seems to miss the fact that many models of anger management are based on group models that rely on CBT frameworks. We use the CBT framework for our anger management groups. Overall I give the article two thumbs up. Kudos to the staff at Yale! Dr. Perna |

Categories All "Dyslexia affects many brain regions, not just those involved with language." 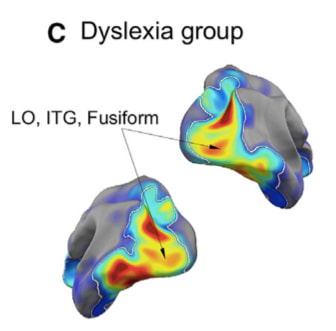 | MIT Researcher John Gabrieli published fascinating findings in the journal Neuron as part of his research and the research of his team (See Reference below) into the roots of dyslexia. His research revealed that dyslexia impacts many different systems within the brain which in turn impact the ability of the dyslexic child to adapt to his/her environment. Gabrieli also noted:
I found this article fits my clinical impressions of the complex nature of many child and adolescent patients who struggle with dyslexia. It also highlights the numerous systems that we need to address in our treatment in an applied clinical setting with this population. In our work, we commonly address the degree to which these patients struggle with anger outbursts, poor frustration tolerance, and impulsivity, all of which bring them to our door for treatment. In treating such a complex population, our treatment interventions are equally complex, including familial support, school support, self-esteem support, referral for specialized testing (Such as Central Auditory Processing Evaluations), and individual/family therapy that are all intertwined to address each patients specific learning/mental health concerns. It is beyond the scope of this review to reveal the complexity of this MIT team's work in this area. A thorough reading of the article that is listed below is recommended. Perrachione et al., 2016, Neuron 92, 1383–1397 December 21, 2016 |
  |  Image From the New York Times |
Categories All | Here is the 2014 New York Times article that many educators have asked me to forward to them. It focuses on the differences in note taking with a pen vs. keyboarding on a computer. It talks about:
Please feel free to look at Dr. Mueller and Oppenheimer's academic article: Mueller, P., & Oppenheimer D. M. (2014). The Pen Is Mightier Than the Keyboard: Advantages of Longhand Over Laptop Note Taking. Psychological Science, Vol. 25(6) 1159–1168
Here is the link to the original New York Times article that was written by reporter Laura Papano: Take Notes From the Pros (2014, October 31) The New York Times, Retrieved From http://nytimes.com | ||
  | Your child's eating is important/ |

"Focus on healthy eating in your home... these healthy habits will follow your | The habits we develop early in life are likely to stick with us throughout our lifespan. This is why it’s important to teach our children right from wrong, daily life skills, appropriate ways to socialize, and a multitude of other skills to help encourage our children to develop healthy adult habits. One skill that tends to get overlooked in families is healthy nutrition habits. Often, when our children are younger, our main goal is to encourage them to eat anything, rather than focusing on the timing and quality of their meals. This is an injustice to our children in various ways. Not only are we neglecting to establish healthy eating patterns in terms of choosing and enjoying healthy foods, but we are also neglecting to teach our children appropriate structure and patterns regarding their eating. Parents can only control what is going on in their home not their neighbor’s homes, therefore, it’s important to model and set these patterns in a realistic way. The end goal is to allow children to generalize these patterns to additional settings without the help of their parents. |

Vocabulary is important... | Introduction to Healthy Foods: Let’s start with their introduction to healthy foods. It is important to remember that we develop the majority of our interests at a young age. This is why parents tend to introduce children to certain sports, activities and books during childhood. The same concept is applicable for food. If parents introduce fruits, vegetables, proteins and grains at a young age, these foods become “normal” and we develop a pattern of enjoyment and acceptance of these foods. Younger children learn the majority of habits through watching others; this process is referred to as social learning. This means that children are constantly watching parents and other adults in order to develop a framework for how to live in the world around them. Therefore, if parents are modeling healthy eating habits, children are likely to follow suit. Sometimes parents are unaware of how closely children scrutinize their eating habits as well as the food s that they eat. There are other options available to model healthy eating habits such as taking your children to the grocery store with you, exploring and learning about new and healthy foods and how to incorporate certain nutrients into your meals, and learning to cook to make meals fun and part of a creative process.. On the other hand, if parents choose to place sugar and various junk foods completely off limits, their children may learn to crave these foods and overindulge in them, i.e., binging on them. They become taboo. Sometimes the pendulum swings too far and extremes aren’t usually realistic to incorporate into everyday life. This is why the concept of balance is most important to healthy eating which is often the case in most other areas of life. Vocabulary is important. Parents should help children understand which foods are healthy “go-to foods,” and those that are considered “snacks.” An active dialogue and ongoing information opportunities builds a child’s knowledge-base of healthy eating. Micromanaging and controlling everything your child eats is simply not okay and is likely to prompt them to build up a sense of resentment and anger. Over time once they have learned realistic and balanced ways to incorporate all foods into their diets, they are less likely to overindulge when left alone. In essence they have incorporated your values around food, and in the end that is what most parents want their kids to do. |

"If we aren’t getting adequate nutrients we can feel lethargic, depressed, anxious or easily agitated" | How Nutrition Affects Mental Health: So, how does healthy nutrition affect our mental health? There are lots of ways nutrition affects our mental health, specifically relating to the way nutrition can affect our brain. Certain nutrients, or lack of nutrients, can either help or hinder the way our brain is working in terms of our energy and our mental capacity to focus.
Therefore, if we aren’t getting adequate nutrients we can feel lethargic, depressed, anxious or easily agitated. Alternatively, if we are getting the proper nutrients throughout the day we are likely to feel energized, motivated and calm. All of these symptoms can be amplified for the better or worse once they are combined with life’s many ups and downs. |
"Eating routines and structure are important." | Structure and Routine: The next important aspect of nutrition is structure and pattern. Life is hectic and for most parents it is difficult to have structured meals on a daily basis. Sometimes parents squeeze in a meal whenever people are home or in between activities. Developing unhealthy eating patterns teach children that eating is not a priority, nor does it require a lot of attention. Under such conditions children learn to avoid planning meals and eating them at set times during the day. As they mature, children can become adults who value nutrition and consistency and appreciate the impact of their nutritional choices on their energy levels and overall health. |
"Role-model how to eat a meal at a reasonable pace." | Nutrition Labels and Meal Pacing: One area of detail that many parents forget is the simple process of modelling how to read nutrition labels in the grocery store. By doing so, we can teach our children how the many details associated with healthy nutrition are easily identified by a quick look. Research has shown that awareness of the overall number of calories in a given food portion can impact a child’s decision to eat it if he/she is aware of how much effort it would take to burn off those calories by walking, running, or biking. Be sure to role-model how to eat a meal at a reasonable pace. Enjoy that first portion of food, relax and chat a bit while eating, and then ask yourself, “Am I still hungry?’ If the answer is yes, then it is okay to have another portion. Remember it takes our stomach about 20 minutes to tell our brain we are full. When we are eating too quickly, we don’t realize we are full until it is too late, therefore, causing overeating. One piece of advice to address this issue at meal time would be to have kids start eating their meal, then introduce a topic for discussion to slow down the eating process. Questions about the school day, a news event, or “high-lows” of the day are generally helpful. After a conversation you can ask your child if he she is still hungry? |
"Mindful eating incorporates the five senses; smell, taste, sound, touch and sight." | The Mindful Meal: Every parent has heard the term “Mindfulness,” but have often been confused about how to apply this concept to life-events. A main component of anxiety reduction treatment is “mindfulness” work. This treatment modality speaks to the notion that as a society we are constantly multitasking and not fully immersing ourselves into what we are doing at any given moment, thus, overwhelming our minds and leading to anxiety and stress. A portion of mindfulness work incorporates mindful eating. As a family, it is important to strive for “The Mindful Meal”. This involves setting aside planned time and concentrating on just the action of eating our meals, without the distraction of any other tasks. Mindful eating also incorporates the five senses; smell, taste, sound, touch and sight. These can all be incorporated by using them as a framework for a discussion around the meal such as:
All of these concepts of mindful eating help train our minds and bodies to be present and calm. When your children and your family is more stress free, you are able to talk amongst yourselves about other things, thus facilitating healthy meals times and healthy discussion within the family. |
References:
http://www.abc.net.au/parenting/articles/nutrition_toolkit.htm
http://www.mentalhealth.org.uk/help-information/mental-health-a-z/d/diet/
http://www.nchpad.org/606/2558/Food~and~Your~Mood~~Nutrition~and~Mental~Health
http://www.livestrong.com/article/480254-how-long-does-it-take-your-brain-to-register-that-the-stomach-is-full/
http://life.gaiam.com/article/zen-your-diet
http://tribecanutrition.com/2013/05/healthy-snacks-around-the-clock-or-structured-meals/
http://www.everydayhealth.com/anxiety-pictures/anxiety-foods-that-help-foods-that-hurt-0118.aspx#10
Categories
All
1 David A. Perna
2 Caitlyn Chappell
Adolescent Psychology
Anger Management
Borderline Personality Disorder
Executive Function
Healthy Lifestyles
Social Media
Technology
Your Child
Youth Violence
 David A. Perna, PhD |  |
"Executive functions are viewed to be primary learning challenges that impact functioning across a variety of learning contexts." | Many children with anger issues suffer from executive function deficits. These deficits impact their ability to make effective academic progress in school in addition to impacting their functioning in a variety of other social-learning contexts. Executive functions are viewed to be primary learning challenges that impact functioning across a variety of learning contexts. Unlike a specific learning disability, such as dyslexia, which is viewed to impact a specific learning category, such as reading, an executive function deficit generally, impacts multiple categories of learning. For example, an attention deficit disorder would impact an individual’s ability to make progress in many learning categories, whether they are academic or social. The inability to pay attention in class can impact the ability to learn history as well as the ability to drive a car safely. Organizational deficits are pervasive as well. For example, the inability to organize one’s assignment pad would impact school performance, while it could also impact the ability to socialize with friends (calling friends to get together too late on a friday night rather than earlier in the week). |
"Cognitive flexibility allows kids to adjust to the curve balls that life throws at them." | Common Executive Function Deficits Associated with Anger Management Disorders: 1. Causal Linking Challenges: The inability to understand that one event causes the other. An example would be a patient who thinks that his probation officer is causing him to have a limited social life, forgetting the fact that the probation officer was assigned to work with him because he had made the poor choice of assaulting another person. In this situation the patient loses track of his own behavior as the primary reason why he has lost many age-appropriate freedoms. Within school it might include the lack of understanding that completing homework will increase one’s understanding of the class material and subsequent performance on tests. 2. Organizational Deficits: Difficulties with the ability to keep track of details that allow the patient to successfully negotiate a myriad of social interactions and learning opportunities. An adolescent might be upset that she has misplaced her homework assignment and cannot complete her homework. However, within her social interactions she might become angry at a parents when she misplaces a slip of paper that contained a phone number that she felt was essential to her social life. 3. Sequencing Challenges: Difficulties with the ability to keep track of sequences of events that are needed to facilitate a positive outcome in a learning situation. The inability to follow a given sequence to solve a math problem will generally result in the wrong answer. In a job situation, an adolescent might sanitize the counters of a fast-food establishment and then place a package with raw chicken onto the cleaned counter in front of his boss just prior to being terminated. A hard-working kid would have lost a job over the likelihood that his sequencing challenge could result in someone going to the hospital. 4. Time Management Issues: Difficulties with allocating time to complete/attend events and activities that are of meaning to the patient or other people in his/her environment. An example would include having an adolescent plan on completing a major project for school on a weekend when relatives were visiting from out of town resulting in a huge family fight. Within the social realm it might include being bombarded by complaints from peers as a result of being late for a movie. 5. Transition Issues: Difficulties with the ability to transition between two activities. Examples of these difficulties range from obvious difficult transitions, such as ending summer and starting school in September to less clear transitions, such as the movement from a sleeping state to a waking state each morning. The resulting morning tirades can be overwhelming for parents. Within a middle school environment the process by which kids constantly move from class to class could prompt a student with this challenge to feel unsettled throughout the school day. As soon as he feels settled in class the bell rings and he has to head off to the next one. As the day progresses the sense of stress increases to the point where an explosion can occur in the last period of the day. 6. Cognitive Flexibility: The ability to learn new ways of coping with ever-changing stressors in a fluid manner. This issue is many times referred to as the ability to be prepared for all of the “Curve balls” that life throws one’s way. A child who was taught one way of solving a math problem using long division in 5th grade becomes enraged when her 6th grade teacher introduces a new method. Or in social settings it might represent the ability to quickly respond to the fickle interests of a peer group who wanted to go to the mall on Friday night when plans were made earlier that day during school lunch, to the movies when plans were made at 6PM Friday night, and out for food at 9PM when all the peers at the theater realized that the popular kids were having dinner at a nearby Shake Shack. For the average teen popularity always tops planning, however, for the teen with cognitive flexibility issues the plan is written in stone. This skill challenge is closely tied to transitioning challenges and challenges in understanding other people’s perspectives (theory of mind). 7. Memory: The ability to remember information in a manner that allows it to be readily available for quick and efficient access. For example, a child might erupt at the thought that he had to get his hair cut when in fact both parents informed him of the hair cut days earlier. In school it might include the embarrassment of walking into class on a Monday morning and being handed a test by the teacher after forgetting to study over the weekend. 8. Generalization: The ability to generalize from one situation to the other. For example, a student is told not to write on his desk at school, which he agrees not to do, but is then caught writing on a table in the cafeteria. In such a situation the child may be incredibly frustrated that the teacher did not clarify this issue to a greater extent and may become highly focused on the fact that he has not written on his desk since the teacher asked him to stop. The connection between the two situations is simply not apparent to the student, while the teacher may start to feel that the student is playing him/her. In reality the student is simply clueless to the connection between the two contexts. |
Categories
All
1 David A. Perna
2 Caitlyn Chappell
3 Heather Corazzini
4 Alexis Chirban
Adolescent Psychology
Anger Management
Borderline Personality Disorder
Cultural Awareness
DBT Techniques
Diversity
Education
Executive Function
Healthy Lifestyles
Learning Challenges
Mindfulness
Nutrition
Social Media
Technology
Your Child
Youth Violence